Table of Contents
Omega-3 and Cholesterol Benefits: Introduction
Omega-3 fatty acids — primarily eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) — are essential long-chain polyunsaturated fats critical to cardiovascular health.
Although omega-3s do not substantially reduce low-density lipoprotein (LDL-C), or “bad” cholesterol, they provide broad cardiometabolic benefits that extend far beyond traditional cholesterol lowering.
Clinical research consistently shows that omega-3s can:
- Reduce triglycerides by 20–30%
- Modestly increase HDL (“good”) cholesterol
- Improve endothelial function
- Lower inflammation and oxidative stress
- Stabilize arterial plaques and support heart rhythm regulation
Together, these effects help prevent and slow the progression of atherosclerosis — the buildup of fatty plaques inside arterial walls — while improving vascular elasticity and overall cardiovascular resilience, especially in individuals with dyslipidemia or elevated cholesterol levels.
Omega-3s and Lipid Metabolism: Beyond LDL Reduction
While lowering LDL cholesterol remains a cornerstone of cardiovascular prevention, research shows that omega-3s act on the quality, not just the quantity, of lipids in circulation.
- Triglyceride Reduction and HDL Improvement: High-dose omega-3 therapy (typically 2–4 g/day of combined EPA + DHA) can lower triglycerides by up to 30% while modestly raising HDL cholesterol. These changes reduce the pool of triglyceride-rich lipoproteins (TGRLs), which are now recognized as independent atherogenic particles — confirmed through large Mendelian randomization studies. (Ference et al., Circulation Research, 2020)
- EPA vs. DHA — Distinct Effects on LDL: Not all omega-3s behave the same:
- EPA-only formulations (e.g., icosapent ethyl) tend to have neutral or beneficial effects on LDL particle size and oxidation, without raising total LDL-C.
- DHA-containing formulations may sometimes cause small increases in LDL-C, though this shift often reflects a conversion toward larger, less atherogenic LDL particles, which are less likely to penetrate arterial walls.
- This distinction underscores why lipoprotein quality — particle size, oxidation state, and function — matters more than total cholesterol numbers alone.
Residual Cardiovascular Risk: When LDL Is Normal but Risk Persists
Many individuals maintain normal LDL-C yet still face elevated cardiovascular risk. This “residual risk” is largely driven by high triglycerides, inflammation, and dysfunctional HDL or LDL particles.
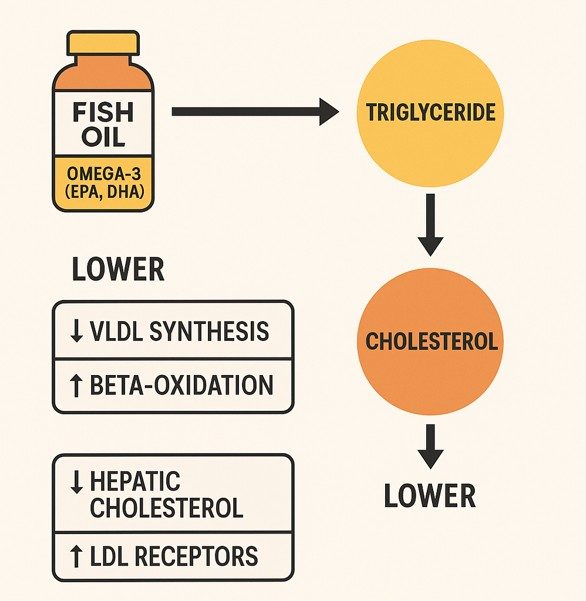
Omega-3 fatty acids—particularly EPA and DHA—provide significant cardiovascular benefits by lowering triglycerides through enhanced fat metabolism and reduced liver synthesis. At therapeutic doses (2–4 g/day), they further protect against atherosclerosis through powerful anti-inflammatory, antioxidant, and endothelial-supporting effects.
A pivotal 2022 study demonstrated these effects in high-risk individuals:
Cartolano et al., Nutrients, 2022 (PMCID: PMC8905646)
- Participants supplementing with 1.8 g/day of EPA+DHA showed increased large HDL particles, reduced small HDL, and lower CETP activity, all indicators of improved HDL efficiency.
- Omega-3 intake also enhanced HDL’s antioxidant enzyme activity (PON1) and improved the balance of apolipoproteins (↓Apo CIII, ↑Apo AI, ↑Apo CII), reinforcing a more protective lipid profile.
Clinical Evidence: Omega-3s in Cardiovascular Outcomes
Study: REDUCE-IT Trial (Bhatt et al., 2019)
The REDUCE-IT study remains one of the most influential omega-3 outcome trials.
In patients with cardiovascular disease or diabetes who were already on statins and had well-controlled LDL-C, supplementation with 4 g/day of pure EPA (icosapent ethyl) led to a 25% reduction in major adverse cardiovascular events (MACE). These results illustrate how omega-3s reduce residual cardiovascular risk even when LDL is “optimal.” (Bhatt et al., New England Journal of Medicine, 2019)
Mechanistic Insights
- EPA incorporation into atherosclerotic plaques improves stability and reduces the risk of rupture — a key trigger of heart attacks and strokes.
- Anti-inflammatory and pro-resolving pathways: EPA and DHA generate Specialized Pro-Resolving Mediators (SPMs) — resolvins, protectins, and maresins — that actively terminate inflammation, support vascular healing, and limit oxidative injury.
- Endothelial and membrane effects: DHA improves cell membrane fluidity, enhancing nutrient exchange and vascular tone, while EPA protects against lipid oxidation and inflammatory signaling.
| Mechanism | Primary Effect | Clinical Impact |
|---|---|---|
| ↓ Triglyceride synthesis | Less hepatic VLDL secretion | 20–30% TG reduction |
| ↑ Lipoprotein lipase activity | Faster clearance of triglycerides | Fewer remnant particles |
| ↑ HDL quality & antioxidant capacity | Improved cholesterol transport | Enhanced reverse cholesterol flow |
| ↓ Apo CIII & ↑ Apo AI/CII | Healthier lipid metabolism | Fewer small, dense LDL particles |
| ↑ Plaque stability & ↓ oxidation | Reduced rupture risk | Lower MACE incidence |
| ↑ SPM production | Resolves inflammation | Improved vascular repair |
EPA vs. DHA: Complementary but Distinct
| Feature | EPA | DHA |
|---|---|---|
| LDL impact | Neutral or lowers oxidized LDL | May raise LDL-C slightly (larger, less atherogenic particles) |
| Oxidative stability | Higher | Lower |
| Anti-inflammatory potency | Stronger | Moderate |
| Neural and visual benefits | Moderate | Stronger |
| Role in plaque stability | High | Moderate |
Takeaway: Combining EPA and DHA offers broad lipid and vascular benefits, while EPA-only formulations may be preferred for targeted triglyceride and plaque-stabilization benefits.
Omega-3 Benefits for Cholesterol: 2025 Insight, Key Takeaways:
– Omega-3 fatty acids may not directly lower LDL-C, but they play a vital role in improving the overall lipid balance and cardiovascular health.
– They significantly reduce triglycerides, enhance HDL functionality, and mitigate inflammation—three mechanisms that work synergistically with LDL-lowering therapies.
– Clinical studies demonstrate that omega-3s improve HDL particle size, composition, and antioxidant capacity, strengthening its role in reverse cholesterol transport.
– On a molecular level, omega-3s lower Apo CIII while increasing Apo AI and Apo CII, indicating deeper improvements in lipid metabolism and lipoprotein function beyond cholesterol numbers.
– High-purity, properly dosed omega-3 supplements are especially beneficial for individuals with mixed dyslipidemia (elevated LDL and triglycerides) or metabolic syndrome, supporting a more protective lipid environment overall.
MVS Omega-3 — Setting a New Standard in Purity, Stability, and Bioavailability
Developed by MVS Pharma’s medical and pharmaceutical experts, MVS Omega-3 represents a new generation of scientifically designed Omega-3 supplements. With a 92% natural rTG structure, verified bioavailability of 1207 mg, and our proprietary T-TOX™ oxidation control system, it ensures exceptional purity, stability, and absorption. Each batch meets European Pharmacopeia standards and is tested for over 20 potential contaminants — setting a benchmark for transparency and trust in modern nutritional science.

Not all Omega-3 supplements are created equal. The more unsaturated and effective Omega-3 molecules become, the more sensitive they are to air exposure — making oxidation protection the single most critical factor for preserving both safety and bioavailability. Once oxidation begins, oil turns rancid, loses efficacy, and may even generate free radicals.
At MVS Pharma, this challenge defined our mission. We engineered MVS Omega-3 as a next-generation formulation designed for uncompromised purity, verified stability, and maximum biological usability.
Key Facts:
- 90% Purified Omega-3 Concentration — delivering 1440 mg total oil with 1312 mg active Omega-3s (EPA 784 mg, DHA 518 mg) per serving.
- 92% Re-esterified Triglyceride (rTG) Form — structurally identical to natural fish oil for superior absorption (1207 mg bioavailable) and full physiological compatibility.
- T-TOX™ Total Oxidation Control System — exclusive German oxidation-management technology ensuring freshness and molecular integrity from production to the last capsule.
- Dual-Layer Packaging Protection — prevents oxidation, preserves hygiene, and guarantees stability throughout the product’s entire lifecycle.
- Ultra Thin Capsule Release 3.0™ — 2/3 less gelatin, no plasticizers, and >91% active ingredient load for transparency, purity, and optimized payload.
- Natural Tocopherol Matrix (α, β, γ, δ) — balanced antioxidant system calibrated to protect high-purity oil without destabilization.
- Pharma-Standard Purification & Testing — each batch is verified to meet European Pharmacopeia standards and is screened for over 20 contaminants, including heavy metals, PCBs, dioxins, PAHs, and plasticizers.
The result is an ultra-pure, oxidation-protected Omega-3 supplement that maintains its natural structure, freshness, and full efficacy until the final dose — ensuring consistent support for cardiovascular, cognitive, visual, and immune health.
Conclusion
Omega-3 fatty acids represent a modern, evidence-backed approach to cardiovascular care — one that looks beyond LDL numbers to lipid functionality, inflammation, and vascular integrity.
- By improving triglyceride control, HDL performance, endothelial health, and plaque stability, omega-3s address the residual cardiovascular risk that persists even after statin or PCSK9 therapy.
- Their benefits are rooted in biochemistry — from enhanced lipid metabolism to resolution of inflammation through SPM pathways. These mechanisms translate to real-world outcomes: fewer heart attacks, improved vascular flexibility, and stronger arterial protection.
For clinicians, omega-3s represent an adjunctive therapy that bridges the gap between nutrition and pharmacology. For consumers, they are a proven, safe, and accessible way to support heart health and long-term lipid balance.
FAQs
Does omega-3 lower bad cholesterol (LDL)?
Not directly. Omega-3s, especially EPA and DHA, primarily work by lowering triglycerides rather than reducing LDL cholesterol. However, they can improve LDL particle quality, making them larger and less atherogenic, which reduces their ability to contribute to plaque buildup — an equally important cardiovascular benefit.
Can omega-3 help increase good cholesterol (HDL)?
Yes. Studies show that omega-3s can modestly increase HDL levels (by about 5–10%) and, more importantly, improve HDL function — enhancing its antioxidant and cholesterol-clearing properties. This helps the body remove excess cholesterol from arteries, supporting long-term heart and vascular health.
How much omega-3 should I take for cholesterol and triglyceride support?
Clinical evidence suggests that taking 2–4 grams per day of combined EPA and DHA can significantly reduce triglycerides and improve overall lipid balance. Always consult your healthcare provider before starting supplementation, especially if you’re on statins or blood-thinning medication.
What’s the difference between EPA and DHA when it comes to cholesterol?
EPA helps stabilize arterial plaques and reduces inflammation without raising LDL levels, while DHA may slightly increase LDL cholesterol but shifts it toward a larger, less harmful particle size. Both are beneficial, but EPA-rich formulations are often preferred for managing triglycerides and cardiovascular risk reduction.
Can I get enough omega-3 from food alone?
Most people don’t. Even those who eat fatty fish regularly often fail to reach optimal omega-3 blood levels (Omega-3 Index ≥8%). While foods like salmon, sardines, and mackerel are excellent sources, high-purity omega-3 supplements ensure consistent intake and reliable cardiovascular benefits.
Is omega-3 safe to take with cholesterol-lowering medications like statins?
Yes — omega-3s are safe and complementary to statin therapy.
In fact, clinical trials such as REDUCE-IT demonstrated that adding purified EPA (4 g/day) to statin therapy reduced major cardiovascular events by 25%, showing that omega-3s can address residual risk left after LDL control.
Why choose MVS Pharma Omega-3?
Because it offers oxidation resistance, superior absorption in rTG form, full safety testing, and double protection packaging — ensuring purity and potency from production to consumption.
References
- Cartolano et al., Nutrients, 2022; PMCID: PMC8905646
- Bhatt et al., NEJM, 2019 – REDUCE-IT Trial
- Ference et al., Circulation Research, 2020
- Mozaffarian & Wu, Progress in Lipid Research, 2011; PMCID: PMC5691715